
Written by Dr. G Harsha Vardhan Reddy, DM Medical Gastroenterology, Consultant Gastroenterologist, Hepatologist & Therapeutic Endoscopist — Adithya Gastro and Liver Care, Manikonda | Medicover Hospitals, Financial District, Hyderabad
If your doctor has
recommended ERCP, it usually means that one of the investigations you've
already had — an ultrasound, a CT scan, or an MRCP — has shown something in the
bile ducts or the pancreatic duct that needs to be assessed or treated
directly. And the most common reaction to that recommendation is: What is this
procedure? Is it a surgery? Do I need to be put to sleep? How long will it
take?
Let me answer those
questions properly, because ERCP is a procedure that's frequently recommended
but rarely explained well to patients before they arrive.
The Anatomy Behind Why ERCP Exists
The liver produces bile — a
digestive fluid that helps break down fats. Bile travels from the liver through
a network of ducts, collecting in the gallbladder, and eventually draining into
the duodenum (the first part of the small intestine) via the common bile duct.
The pancreas also has a duct — the pancreatic duct — that carries digestive
enzymes into the duodenum. Both ducts share a small common opening in the
duodenal wall called the ampulla of Vater.
When this ductal system
gets blocked, infected, narrowed, or damaged, symptoms develop: jaundice,
severe abdominal pain, fever, dark urine, pale stools. These are the situations
where ERCP becomes relevant.
Before ERCP existed, most
problems in the bile and pancreatic ducts required open surgery. ERCP replaced
surgery for the majority of these conditions, and has been the standard
approach for over 40 years.
What ERCP Actually Is
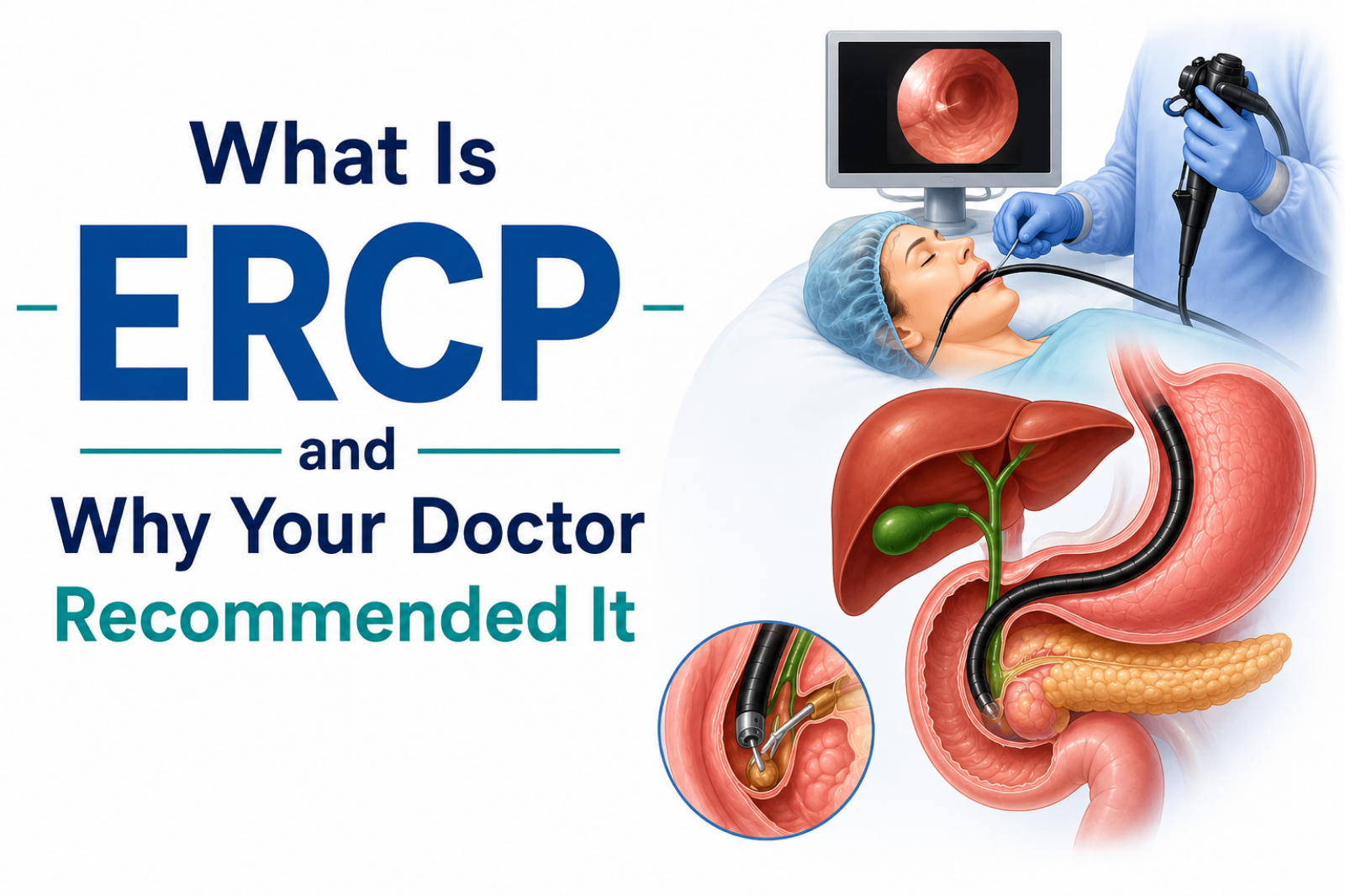
ERCP stands for Endoscopic
Retrograde Cholangiopancreatography. It's a procedure that combines endoscopy —
looking inside the gut with a flexible tube and camera — with fluoroscopy,
which is real-time X-ray imaging.
The word 'retrograde'
refers to direction: instead of flowing forward (from liver to intestine), the
procedure works backward, accessing the bile and pancreatic ducts from the
duodenal end.
Here is what happens, step
by step:
1.
You are given a sedative or
light general anaesthesia. You will not feel pain during the procedure.
2.
A specialised endoscope —
called a side-viewing duodenoscope — is passed through the mouth, down the
esophagus, through the stomach, and into the duodenum.
3.
The opening where the bile
and pancreatic ducts drain into the duodenum (the ampulla) is identified.
4.
A thin plastic tube
(cannula) is threaded through the endoscope and guided into the duct. A
contrast dye is injected so that the ducts become visible on the fluoroscopy
X-ray screen.
5.
Once the problem is located
— a stone, a stricture, a blockage — the necessary intervention is performed
through the endoscope using specialised instruments.
What Can ERCP Actually Treat?
ERCP is not just a
diagnostic tool. In most cases I perform it, it is simultaneously treating the
problem that was identified. The main therapeutic applications are:
Bile duct
stone removal
Gallstones that slip out of
the gallbladder and lodge in the common bile duct are the most common reason
for ERCP. Once inside the duct, these stones can cause blockage, infection,
pancreatitis, and jaundice. During ERCP, I perform a small cut in the sphincter
at the ampulla (called a sphincterotomy), then use a balloon or basket to
extract the stone. Most stones are removed in a single session. Larger or more
complex stones may require mechanical lithotripsy — essentially crushing the
stone before removal.
Biliary stent
placement
When the bile duct is
narrowed due to a tumour, cancer, stricture, or external compression — and
opening it surgically is either not possible or not yet planned — a plastic or
metal stent can be placed through ERCP to hold the duct open and allow bile to
drain. This relieves jaundice, reduces infection risk, and significantly
improves quality of life. Metal stents are preferred for malignant obstruction;
plastic stents are used for benign strictures and can be replaced.
Biliary
sphincterotomy
Cutting the sphincter to
improve drainage. Done as part of stone removal or to treat sphincter of Oddi
dysfunction, which is a cause of recurrent unexplained abdominal pain.
Management of
bile leaks
After gallbladder surgery
(laparoscopic cholecystectomy), bile can sometimes leak from the cystic duct
stump or an accessory bile duct. ERCP with stent placement closes the leak from
the inside, avoiding a return to surgery.
Pancreatic
duct drainage
In chronic pancreatitis
with pancreatic duct stricture or stones, ERCP can dilate the stricture or
remove the stones, relieving pain and reducing recurrent attacks. In some
cases, a pancreatic duct stent is placed to maintain drainage.
Tissue
sampling (biopsy)
If an abnormality — a
stricture, a filling defect, a suspicious area — is seen in the ducts during
ERCP, a small tissue sample can be taken through the scope for histological
analysis.
What ERCP Feels Like: Before, During and After
Before the
procedure
You will fast for at least
6 hours beforehand — nothing to eat or drink. If you are on blood thinners,
your doctor will advise on whether and when to pause them. Antibiotics may be
given beforehand, particularly if infection is a concern. Someone needs to
accompany you and take you home afterward, as the sedation takes several hours
to fully wear off.
During the
procedure
Most patients have no
memory of the procedure itself, or only a vague sense of movement. The sedative
— propofol or midazolam with pethidine — keeps you comfortable throughout. The
procedure takes between 30 and 90 minutes depending on what is being treated.
If a sphincterotomy and stone removal are both needed, it will be longer than a
simple diagnostic ERCP or stent placement.
After the
procedure
You will be observed for 2
to 4 hours in the recovery area. Most patients are discharged the same day. If
the procedure was complex, or if there is any concern about post-procedure
pancreatitis, you may be kept overnight. Mild bloating and a sore throat from
the endoscope are common and settle within a day. You will be asked to stay on
a liquid or light diet for the rest of the day.
What Are the Risks?
ERCP has a strong safety
record, but it is a more complex procedure than a standard endoscopy and
carries specific risks that patients should know about:
•
Post-ERCP pancreatitis —
the most common complication, occurring in approximately 3–5% of cases. Usually
mild and managed with IV fluids and monitoring. Severe pancreatitis is rare but
can occur.
•
Bleeding — particularly
after sphincterotomy. Uncommon, and usually manageable endoscopically.
•
Cholangitis — bile duct
infection. Risk is higher in patients with pre-existing biliary obstruction.
Treated with antibiotics and, if necessary, repeat drainage.
•
Perforation — very rare.
The risk profile depends on
the specific indication, the patient's baseline health, and the complexity of
the procedure. I discuss this individually with every patient before
proceeding.
ERCP at Medicover Hospitals, Financial District
I perform ERCP and the full
range of therapeutic biliary endoscopy at Medicover Hospitals, Financial
District, Hyderabad. Patients come from across Hyderabad and are referred by
gastroenterologists, general physicians, surgeons, and hepatologists who need
their patients to have the procedure done by someone with specific
interventional endoscopy experience.
If you have been told you
need ERCP — or if you have a bile duct, gallstone, or pancreatic duct problem
and want to understand what treatment involves — a consultation at Adithya
Gastro Manikonda or at Medicover Financial District is the right starting point.
Call or WhatsApp +91 63038
38583 to book a consultation.
Frequently Asked Questions
1. Is ERCP a
surgery?
No. ERCP is an endoscopic
procedure — it is performed through the mouth using a flexible endoscope, with
no incisions in the skin. It is done under sedation, not under general
anaesthesia in most cases, although some centres including ours use monitored anaesthesia
for patient comfort.
2. How long does
ERCP take?
Most ERCP procedures take
between 30 and 90 minutes. A straightforward stent placement may be done in
under 30 minutes. A difficult stone removal or a procedure involving both
sphincterotomy and extraction may take longer.
3. How long is
recovery after ERCP?
Most patients are
discharged the same day and return to normal activity within 1–2 days. You
should not drive on the day of the procedure due to sedation.
4. Can ERCP be
done without an overnight hospital stay?
In most straightforward
cases, yes — ERCP is a day procedure. Overnight observation is recommended when
the procedure was complex, when the patient has significant comorbidities, or
when there is any concern about post-procedure pancreatitis.
5. Is ERCP
available at Medicover Hospitals Financial District?
Yes. I perform ERCP at
Medicover Hospitals, Financial District, Hyderabad. Patients from Manikonda,
Gachibowli, Kondapur, Kokapet, Narsingi, and across Hyderabad can be seen for
consultation at the Manikonda clinic or directly at Medicover.
6. What should I tell my doctor before having ERCP?
Inform your doctor of all
current medications, particularly blood thinners (aspirin, warfarin,
clopidogrel, rivaroxaban), diabetes medications, and any allergies — especially
to contrast dye. Also mention any prior surgery on the stomach, duodenum, or bile
duct, as this affects the approach.
